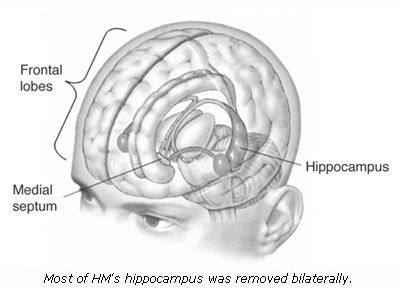
Last week, Henry Gustav Molaison -- a name most would not recognize even though he was the neuroscience field's most famous of patients -- passed away at the age of 80. Since 1953, when experimental brain surgery to alleviate severe epileptic seizures severely damaged his ability to lay down new memories, Molaison was known simply as "H.M."
From Wikipedia:
Henry Gustav Molaison (February 26, 1926 – December 2, 2008), better known as HM or H.M., was a memory-impaired patient who was widely studied from the late 1950s until his death. His case played a very important role in the development of theories that explain the link between brain function and memory, and in the development of cognitive neuropsychology, a branch of psychology that aims to understand how the structure and function of the brain relates to specific psychological processes.
Before his death, he resided in a care institute located in Windsor Locks, Connecticut, where he was the subject of ongoing investigation. Audio recordings from the 1990s of him talking to scientists were released in early 2007. Henry loved to do crossword puzzles, play bingo, watch TV, and socialize with the people who took care of him.
Not surprisingly, in February 2007, NPR's Weekend Edition [
listen] introduced their audience to the man whose ill-fated surgery gave scientists a clearer window into the body's most complex and vital organ: the brain. The program also provides a short introductory primer on memory and the brain.
Due to PTSD and memory's unique relationship -- with past traumatic experiences feeling vivid, painfully immediate and even more "real" than recent events rather than the distant memories they should be for its sufferers -- H.M. (who was an "
n of 1," or the only person who is known to have had the surgical procedure performed on him; therefore, the only one available in this specific research pool) increased our knowledge base in this area, too.
In extended, a journey into the world of Molaison's amnesia, along with a host of fresh research coming out on the subject.
 Veterans for America delivers an early holiday present to our nation's military families: "The American Veterans’ and Servicemembers’ Survival Guide," a 599-page guidebook every veteran should own. And there's no need to worry about being naughty or nice, because the VFA Santa has made the ebook available to everyone as a free download.
Veterans for America delivers an early holiday present to our nation's military families: "The American Veterans’ and Servicemembers’ Survival Guide," a 599-page guidebook every veteran should own. And there's no need to worry about being naughty or nice, because the VFA Santa has made the ebook available to everyone as a free download.


 Tomorrow -- Wednesday, December 10 -- is the last day to participate in the Red Cross Holiday Mail for Heroes program. The program is a "
Tomorrow -- Wednesday, December 10 -- is the last day to participate in the Red Cross Holiday Mail for Heroes program. The program is a " Interesting developments in the the current updating of the DSM-IV, or Diagnostic and Statistical Manual of Mental Health Disorders (generally considered the "Bible of Psychiatry"), and the ongoing push to make the process as transparent as possible.
Interesting developments in the the current updating of the DSM-IV, or Diagnostic and Statistical Manual of Mental Health Disorders (generally considered the "Bible of Psychiatry"), and the ongoing push to make the process as transparent as possible.


